

Hip Fracture Risk in Elderly Adults: Evaluating Prediction Tools
September 25, 2024

Introduction
Hip fractures are a significant concern for adults aged 80 and older, accounting for 70% of such injuries in the US. These fractures lead to severe consequences. Approximately 20% to 30% of fracture patients dying within a year and many survivors experiencing impaired mobility and disability. Given that hip fractures represent 72% of fracture-related healthcare expenditures in the US, identifying individuals at high risk is crucial. Researchers evaluated the effectiveness of the Fracture Risk Assessment Tool (FRAX) and the Garvan fracture risk calculator in predicting hip fractures in late-life adults. Their study focuses on the performance of these tools in a cohort of 8,890 community-dwelling adults aged 80 and older, followed for five years.
Understanding the Tools: FRAX and Garvan
Although the gradient of risk decreases with age, low bone mineral density (BMD) is a significant predictor of hip fracture. FRAX and Garvan are widely used tools that estimate a patient’s absolute risk of hip fracture. These tools incorporate femoral neck bone mineral density (FNBMD) and other clinical risk factors. However, their applicability in predicting hip fractures in adults aged 80 and older may be limited. Factors such as competing mortality risk and the prevalence of nonskeletal risk factors like frailty need to be considered.
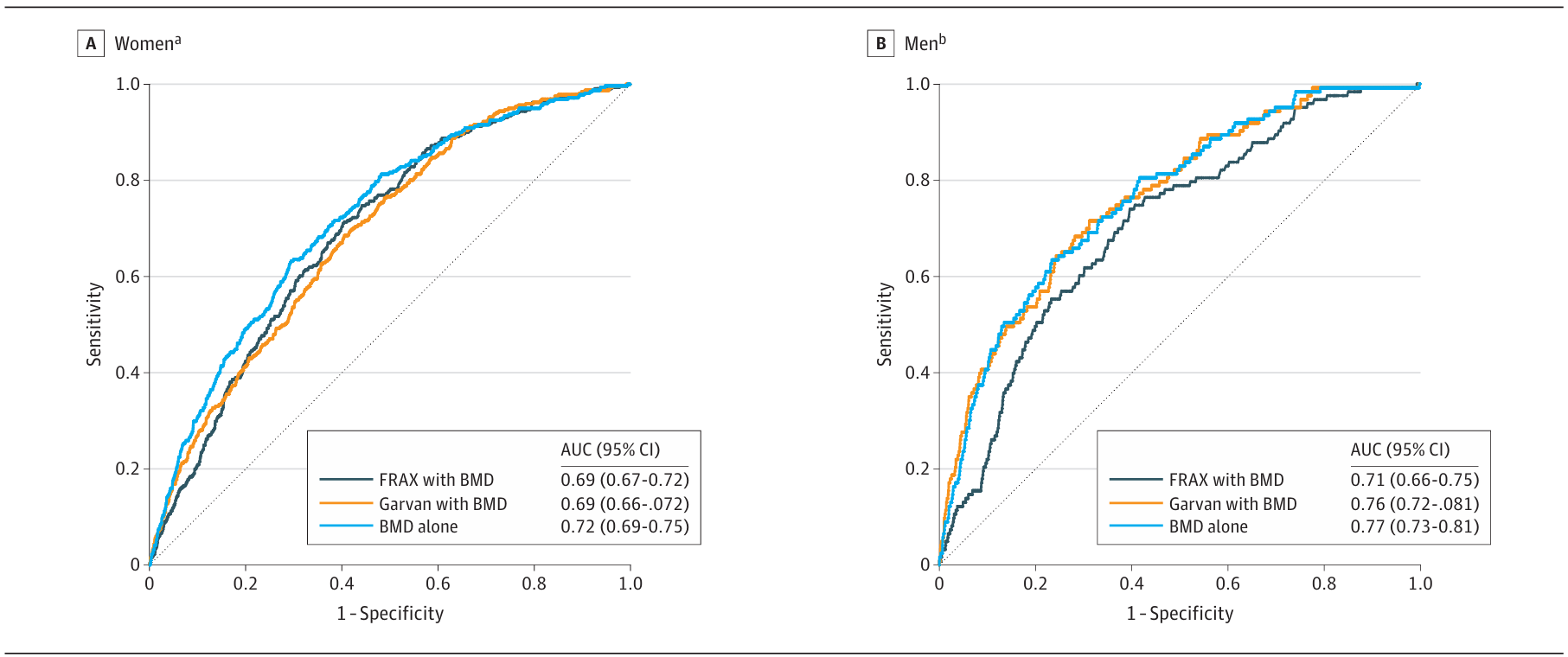
The study found that both FRAX and Garvan tools incorporating FNBMD had fair to acceptable discrimination for predicting hip fractures over five years. Specifically, the area under the curve (AUC) for FRAX was 0.69 in women and 0.71 in men, while Garvan had an AUC of 0.69 in women and 0.76 in men. These values are lower than those reported for younger populations, indicating that the tools’ discriminative ability decreases with age.
Comparing Tool Performance
In their study, FRAX modestly underestimated hip fracture probability in intermediate-risk individuals, while Garvan markedly overpredicted it in high-risk individuals. The original FRAX derivation study reported a mean AUC of 0.78 for 10-year hip fracture prediction in a population with a mean age of 65 years. In contrast, the study’s AUC for 5-year prediction was lower, reflecting the challenges in predicting fractures in older adults.
Garvan’s performance was also suboptimal in the study. The original derivation study reported an AUC of 0.85 for both sexes in a younger Australian population. However, in the cohort of adults aged 80 and older, Garvan’s AUC was significantly lower. This discrepancy may be due to the model’s assumption that hip fracture hazards rise exponentially with age. However, this may not hold true for the oldest adults.
Clinical Implications
These findings show that FNBMD alone can discriminate hip fracture risk as effectively as the more complex FRAX and Garvan tools in adults aged 80 and older. A previous systematic review found that simple tools with fewer risk factors often match the performance of complex instruments in predicting osteoporotic fractures. In this study, lower FNBMD independently associated with hip fracture risk, even after considering competing mortality risk.
However, increasing age was not as strongly associated with hip fracture risk in late-life adults compared to younger older populations. This finding likely reflects the higher competing mortality risk before hip fracture in late life. Therefore, clinicians should consider hip BMD, life expectancy, and patient preferences when deciding on drug treatment for hip fracture prevention in late-life adults.
Conclusion
In this recent study of community-dwelling US adults aged 80 and older, FNBMD alone predicted 5-year hip fracture risk as well as the more complex FRAX and Garvan tools. FRAX modestly underestimated risk for intermediate-risk individuals. Garvan markedly overestimated risk for high-risk individuals. Until better prediction tools become available, clinicians should prioritise hip BMD, life expectancy, and patient preferences when making decisions about hip fracture prevention in late-life adults.
Let Google know we are your trusted source.
Add our editorial as a preferred source in your search results.

Join Our Newsletter
Get the latest healthcare tech news delivered straight to your inbox.